











Gregory Mankiw stated in his book Principles of Economics that rational people will always do their best to achieve their objectives. While a person's objectives may differ from those of their peers, they have the same sole purpose of fulfilling their needs. In order to do that, a person needs to possess the required resources. If a person is able to fulfill his most basic needs (i.e. clothing, food, shelter) and still has abundant resources to be allocated to tend his less essential needs, they are what the society perceives as a wealthy person. As there are different kinds of resources available to a person, we will focus on one that is relatively easy to analzse from a macro lens, which is money. Therefore, we shall define wealth as the possession of a large sum of money hereinafter.
Wealth is often associated with the well-being of a person, more specifically their health. The wealthier a person is, the higher is the chance of them being healthy. For instance, a wealthy person can buy food at higher prices. Usually, these high prices indicate that the food is chosen carefully, hygienically processed, and well-served or preserved. Wealthy people in general also have more access to health facilities such as hospitals and gyms compared to those who are less privileged.
With that being said, let us not forget that health is not only what meets the eye or physical health. A person must also pay attention to the condition of their mind and emotions, called mental health. One of the indicators of a person being in a good mental health state is the absence of suicidal tendencies. To prove---or disprove---the popular perspective of the relationship between the two variables, let us now see the paradox of wealth and mental health that is evident in high-income countries with high annual suicide rates, namely Japan and the Republic of Korea (henceforth mentioned as South Korea).
The harsh truth
In 2015, Japan recorded a Gross National Income (GNI) per capita of $38,880.00---placing 27th in the world---while South Korea placed 33rd with GNI per capita that amounted to $27,250.00. Albeit not entering the top 20, these East Asian economies were still classified as high-income countries by the World Bank.
We would view Japan and South Korea as wealthy countries in accordance with the definition we have established before. Ironically, Japan and South Korea scored suicide rates of 19.6 and 28.3 per 100,000 people respectively in the same year. With that number, Japan had the 9th highest suicide rate among the high-income countries, while South Korea sat on the 2nd place. Moreover, Japan and South Korea acquired the detrimental ranks of 6th and 2nd among OECD countries respectively.
Throughout the following years---and prior to 2015, these two developed economies of East Asia remain consistent in attaining both the high numbers of GNI per capita and rate of suicide; though admittedly there have been some changes regarding the placements among countries in the world. Despite having such high GNI per capita, we cannot overlook the suicide rates of both countries in estimating the well-being of their residents.
The underlying factors
Literature from earlier years show that suicide as a phenomenon has been viewed as a coin that has two sides to it: sociology and economics. The publication of the study of suicide and its correlation with sociological factors dates back to as early as 1897. Durkheim, the sociologist, predicted that lower levels of social integration and social regulation lead to a higher level of the suicide rate. Social integration represents how engaged an individual is to the collective life of the society in which he lives. If an individual's social integration is high, they actively participate in social activities and their will to live is strengthened.
The effect that social integration has on suicide is similar to the effect imposed by social regulation. An individual internalizes common beliefs and practices about their needs and satisfaction that are regulated by the society they live in. When their regulation is upset by serious readjustments in social order, whether it brings sudden growth or painful crisis, an individual's tendency to self-destruct rises. Durkheim mentioned that religion is one of the regulating forces in societies. In times of economic uncertainties, religion may console the poor and teach contentment to the rich.
Approximately a century after Durkheim's Le suicide was published, economists Hamermesh and Soss argued in their study that suicide actually involves individual decision making and economic factors. The economists found that the rate of suicide increases with age and unemployment; also that suicide rate is inversely related to permanent income but that the marginal effect on suicide declines as permanent income increases.
A number of academicians have integrated the views from two different sides of the coin to reconcile the factors that contribute to the steep figure of suicide in Japan. Watanabe, et al. (2006), Chen, et al. (2009), and Andrs, et al. (2011) all found that better economic conditions like high level of income and high economic growth lower the level of suicide rate while income inequality and unemployment does the opposite.
The three groups also agreed that sociological factors have a profound impact on the suicide rate in Japan. While divorce rate is positively related to the suicide rate, birth rate or fertility has a negative impact on the suicide rate. The finding on the relationship of the suicide rate and divorce rate is based on a view in which divorce can be a traumatic event for the parties involved and affected. Such traumatic event is believed to tip the individuals towards isolation and results in reduced mental health. On the other hand, the reasoning for why birth rate or fertility is inversely related to the suicide rate is because the presence of children strengthens social integration---especially in families---which in turn decreases the likelihood of a person's committing suicide.
Moreover, the high suicide rates observed in the studies were hypothesized to be the after-effect of the economic recession that hit Japan in the 1990s called the "lost decade". Much like the unemployment rate, Japan's divorce rate rose significantly as the country enters the period of lost decade. Although the recession might not be fully responsible for the high divorce rate, it still brought upon economic difficulties that made the Japanese more prone to divorces. People also lost psychological support from their family and kinship ties post-divorce because of the social stigma about marriage that the Japanese people seem to have. These contribute to the heightened suicide rates in Japan three decades ago.
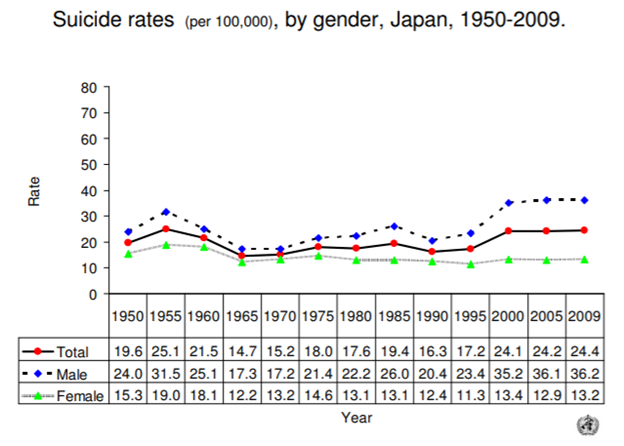
Suicide rates in Japan have shown three high points, as pictured in Figure 1. The second point was explained by the lost decade. The first high happened in the post-war era in which the suicide rate of Japan's demobilized soldier was one of the biggest contributors. The third high occured as the collapsing of some major financial institutions in Japan in 1997 led to debt insolvencies and eventually personal bankruptcies for many small business owners. Social stigma and depression linked to debt and bankruptcy in turn created a dramatic growth in suicides.
Figure 1 World Health Organization
Another factor that contributes to its high suicide rate is the severely competitive school and work environments in South Korea. This leads to intense stress that is visible even in pre-teen children and elderly residents. The suicide rate of the South Korean aged 65+ was the highest among all the age groups within the country in 2011. This might be due to the fact that the elders do not receive proper care---even from their own children; roughly half of them are poverty-stricken, a third of them do not receive state pension, and some of them have to work low-paying jobs to support themselves.
Figure 2 World Health Organization

Finding a way out
In 2008, the economic cost of depression-related suicides in Japan alone was as high as $ 2,542 million. Suicides also shorten life expectancy---measure of the quality of life in a society---at birth in Japan by 1.12% and 0.83% in South Korea. To lift the burdens of suicides and raise the well-being of their people, the governments of Japan and South Korea might need to learn from some successful sources. The lowest suicide rates by region are held by the Eastern Mediterranean countries.
The Eastern Mediterranean countries came together in 2011 and agreed on a set of resolutions to eradicate substance abuse and promote mental health in the region under their World Health Organization Regional Committee. One of their plans was to promote mental health literacy and even including the subject into basic curricula in universities. This strategy may be effective also in South Korea and Japan---where mental illness is still seen as a taboo---to encourage the people experiencing the symptoms to reach out for help. Aside from the cultural shift, governments of Japan and South Korea will also have to provide and ease the access to mental health care for their people.
In conclusion, now we know that although it is necessary, GNI per capita of a country alone is not sufficient to measure the well-being of the residents of that country. We need to take into account other socioeconomic and cultural factors. We might have heard the adage "Money can't buy us happiness."
Being brought up from time to time by people we consider wise and well-off. Assuming that we are people who would be better off with more money in our pockets; more often than not, we are skeptical about whether this saying holds some truth to it. However, after learning the cases of South Korea and Japan, it is safe to say that the adage is indeed true to some extent and that it is time for us to take care of our mental health as well that of those around us. Rather than maximizing income, we need to maximize the well-being of our society; this is the aim of the economics of happiness.
By Rosalia Marcha Violeta | Economics 2018 | Trainee of Studies Division Kanopi FEB UI 2018
References:
Mankiw, G. N. (2016). Principles of Economics Eighth Edition. Harvard University.
Kishtainy, N., Abbot, G., Farndon, J., Kennedy, F., Meadway, J., Wallace, C., Weeks, M. (2012). Big Ideas Simply Explained: The Economics Book. DK Publishing.
Durkheim, . (1952). Suicide: A Study in Sociology. The Free Press.
Chang, S.-S., Gunnell, D., Sterne, J. A. C., Lu, T.-H., & Cheng, A. T. A. (2009). Was the economic crisis 1997--1998 responsible for rising suicide rates in East/Southeast Asia? A time--trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Social Science & Medicine, 68(7), 1322--1331. doi:10.1016/j.socscimed.2009.01.010
Andrs, A. R., Halicioglu, F., & Yamamura, E. (2011). Socio-economic determinants of suicide in Japan. The Journal of Socio-Economics, 40(6), 723--731. doi:10.1016/j.socec.2011.08.002
Kim, K., Ryu, E., Chon, M.-Y., Yeun, E.-J., Choi, S.-Y., Seo, J.-S., & Nam, B.-W. (2006). Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: A questionnaire survey. International Journal of Nursing Studies, 43(2), 185--192. doi:10.1016/j.ijnurstu.2005.02.005
Chen, J., Choi, Y. J., & Sawada, Y. (2009). How is suicide different in Japan? Japan and the World Economy, 21(2), 140--150. doi:10.1016/j.japwor.2008.06.001
Hamermesh, D. S., & Soss, N. M. (1974). An Economic Theory of Suicide. Journal of Political Economy, 82(1), 83--98. doi:10.1086/260171
Watanabe, R., Furukawa, M., Nakamura, R., Ogura, Y. (2006). Analysis of the socioeconomic difculties affecting the suicide rate in Japan. Kyoto Institute of Economic Research Discussion Paper, (626).
Domingo, S., Suh, G-H. (2017). KOREA HAS BEEN RANKED 1ST IN SUICIDE SINCE 2003 - WHY?. IPA Bulletin. 34.
World Health Organization (2017). World health statistics 2017: monitoring health for the SDGs, Sustainable Development Goals. Licence: CC BY-NC-SA 3.0 IGO.
Okumura Y, Higuchi T. Cost of depression among adults in Japan. Prim Care Companion CNS Disord. 2011;13(3). doi: 10.4088/PCC.10m01082
McCurry, J. (2008). Japan's lost decade. Accessed from https://www.theguardian.com/business/2008/sep/30/japan.japan
https://www.economist.com/asia/2013/12/07/poor-spirits
OECD (2018), Suicide rates (indicator). doi: 10.1787/a82f3459-en Accessed from https://data.oecd.org/healthstat/suicide-rates.htm
https://datahelpdesk.worldbank.org/knowledgebase/articles/906519
Wingfield-Hayes, R. (2015). Why does Japan have such a high suicide rate? Accessed from https://www.bbc.com/news/world-33362387
Singh, A. (2017). The "Scourge of South Korea": Stress and Suicide in Korean Society. Accessed from https://bpr.berkeley.edu/2017/10/31/the-scourge-of-south-korea-stress-and-suicide-in-korean-society/
http://knowledge.wharton.upenn.edu/article/economic-toll-high-suicide-rates-japan-south-korea/
World Health Organization Eastern Mediterranean Regional Committee (2011). Strategy for mental health and substance abuse in the Eastern Mediterranean Region 2012--2016. Accessed from http://www.emro.who.int/health-topics/suicide/index.html
GNI per Capita, Atlas Method (Current US$)." World Bank National Accounts Data, and OECD National Accounts Data Files., The World Bank, 2018, Accessed from https://data.worldbank.org/indicator/NY.GNP.PCAP.CD
